
Stop Testing Your Testosterone. It's Telling You Almost Nothing.
Why your testosterone, DHT, and estrogen levels tell you almost nothing about what’s actually happening in your body and what does.

The Hormone Test Everyone Gets Is Basically Useless
There is a ritual happening thousands of times a day in men’s health communities across the internet.
Someone posts a picture of their bloodwork. Testosterone: 800 ng/dL. DHT: 450 pg/mL. Estradiol: 22 pg/mL. The comments flood in. “Your T is great.” “DHT looks solid.” “E2 is perfect.” The person feels validated. They adjust their protocol based on what they see. They optimize around these three numbers like they are the whole story.
They are not the whole story. They are barely the opening sentence.
What if I told you that two men with identical testosterone, DHT, and estradiol levels could have completely different hormonal realities? Different androgenic loads in their tissues, different estrogen metabolism profiles, different risks, different responses to the same interventions.
And that standard bloodwork would never reveal this?
What if I told you that my wife, a woman on a fraction of the testosterone level I have, has a higher androgen-producing enzyme activity than I do and that her total androgen pool and estrogen pool are nearly the same size as mine? 🤯
What if the entire framework most people use to understand their hormones is missing most of the picture?
That is what this article is about. By the end of it, you will never look at a testosterone panel the same way again.
The Map Is Not the Territory
Before we get into the numbers, we need to establish one idea that everything else builds on.
Hormones are not static chemicals floating in your blood waiting to be measured. They are dynamic signaling molecules that travel through blood as a transport medium, get converted by enzymes in specific tissues, bind to receptors inside cells, drive gene expression and biological function, and then get broken down and cleared by the liver and kidneys.
Every stage of this process is biologically meaningful. Every stage produces measurable outputs. And every commonly used hormone test measures only one stage while ignoring the rest.
Blood testing measures what is in transit at that given time of day.
Saliva testing measures what specific glands secrete.
Urine testing measures what the liver and kidneys have processed and cleared.
And the stage where hormones actually do their work (inside the target tissues, at the receptor level, in the prostate and scalp and brain and muscle) that stage is essentially invisible to all of them.
You are always looking at a shadow of the process, not the process itself. The question is which shadow is most informative for the question you are actually trying to answer.
You’ve spent hours researching. You’ve read the studies. They contradict each other. The experts disagree. And you still don’t know what to actually do.
I’ve spent 10 years, hundreds of lab tests, and thousands of dollars figuring this out on myself, not in theory. On my own blood, my own gut, my own hormones.
Ask Hans gives you access to all of it. Instantly.
No more research. No more confusion. Just ask.
What Blood Testing Actually Measures
When you get a blood hormone panel, here is what is physically happening: a needle draws blood from a vein at a specific moment in time, a lab measures the concentration of specific hormones in that sample, and you get a number.
That number tells you how much of that hormone was circulating in your blood at that particular moment. Nothing more.
This sounds straightforward until you understand the limitations.
Testosterone fluctuates by 25 to 40 percent across a single day. A morning draw and an afternoon draw on the same person under the same conditions can produce results that differ enough to change clinical interpretation. Which number represents your testosterone? Both of them do. Neither captures the full picture.

Serum DHT tells you almost nothing about 5-alpha reductase activity. This is perhaps the most widely misunderstood fact in hormone optimization. DHT in blood is testosterone that has been converted by the enzyme 5-alpha reductase somewhere in the body and then released into circulation. But 5-alpha reductase does not primarily operate in blood, it operates inside tissues.
The prostate converts testosterone to DHT locally. So does the scalp. So does the skin. So does the liver. So does the brain. Most of that locally-produced DHT never enters circulation in proportion to how much was produced. It acts locally and gets metabolized locally.
What appears in your serum is a downstream reflection of a fraction of total 5AR activity, confounded by how much testosterone was available as substrate, how active aromatase was competing for that same substrate, and how efficiently your liver is clearing DHT metabolites.
The T:DHT ratio (the metric people obsess over when trying to assess 5-alpha reductase activity) is measuring three different biological processes simultaneously and cannot distinguish between them. Although the T:DHT ratio is helpful to look at, it also has severe limitations. A low T:DHT ratio could mean 5AR is highly active. It could mean aromatase is less active, leaving more testosterone available for 5AR conversion. It could mean DHT clearance is slower. You cannot tell from the ratio alone.
Estradiol as a single number tells you almost nothing about your actual estrogen health. This is where the picture gets significantly more complicated, and significantly more interesting. Estradiol is one molecule. The body metabolizes estrogens through a cascade of enzymatic steps that produces at least sixteen distinct measurable metabolites, each with different biological activity, different health implications, and different responses to intervention.
Two people with identical serum estradiol can have completely different estrogen metabolism situations, one routing through the safest metabolic pathway, one accumulating metabolites associated with increased cancer risk and inflammatory activity. Standard bloodwork cannot distinguish between them because it only measures the starting point, not where the estrogen goes after.
The Saliva Testing Limitation
Salivary hormone testing has one genuine advantage over blood testing: it primarily captures the free, biologically active fraction of hormones rather than the total including protein-bound forms. Since only unbound hormones can cross the salivary gland epithelium, saliva gives you a reasonable approximation of free hormone levels without the calculation required to estimate free fractions from serum.
For cortisol specifically, salivary testing is well-validated and genuinely useful. The cortisol awakening response (the rapid spike in the 20 to 30 minutes after waking that reflects HPA axis health and morning energy regulation) is best captured in saliva because of its sensitivity to the acute dynamics that a single blood draw misses.
Plus, you also see the daily fluctuations of cortisol and DHEA, not just one static number as with a blood test.
For sex hormones, the picture is less clear. Salivary sex hormone reference ranges are less standardized across laboratories than serum ranges, and the relationship between salivary concentrations and tissue hormone activity is less well characterized.
But the fundamental limitation is the same as blood testing. Saliva tells you about what a specific glandular secretion contains at a specific moment. It does not tell you about enzyme activity, metabolite production, phase II detoxification capacity, or what is happening inside target tissues. It is a different window onto the same transport-phase measurement problem.
The Thing No Test Can Tell You: What Happens Inside Your Tissues
Here is where it gets genuinely important and where most hormone content completely fails to go.
Your prostate does not care what your serum DHT is. Your scalp follicles do not respond to your blood testosterone level. Your brain’s neurosteroid environment is not determined by what is circulating in your bloodstream. Each of these tissues has its own local enzyme activity, its own capacity to convert circulating testosterone into DHT or other metabolites, its own receptor density, and its own hormonal microenvironment that operates semi-independently of systemic circulation.
The evidence for how dramatically tissue DHT can diverge from serum DHT comes from a source most people would not expect: the pharmaceutical literature on finasteride.
Finasteride is a well-characterized 5-alpha reductase type 2 inhibitor. It reliably reduces serum DHT by 65 to 70 percent. By serum metrics, it does exactly what it is supposed to do. But look at what happens at the tissue level.
In the prostate, DHT concentrations in healthy males are naturally 5 to 10 times higher than serum DHT. The prostate is a DHT-concentrating organ with extremely high local 5AR expression and androgen receptor density. Serum DHT tells you essentially nothing about intraprostatic DHT. This is why finasteride was developed for benign prostatic hyperplasia. The target was intraprostatic DHT, and serum measurement was used only as a proxy for drug exposure, not as the meaningful endpoint.
In penile tissue, finasteride produces substantially greater DHT suppression than serum levels suggest, and recovery of penile tissue DHT after stopping the drug lags significantly behind serum DHT normalization. In some cases testosterone even goes up, yet these men develop ED, due to low DHT-induced changes such as reduced eNOS and smooth muscle cells as well alterations in neurotransmitters involved in erections namely noradrenaline and adrenaline (think shrunken flaccid) (R). Men can have fully recovered serum DHT while penile tissue DHT remains suppressed. This is mechanistically relevant to the sexual side effects some men experience, and it is invisible to blood testing.
In cerebrospinal fluid, the findings are the most striking. Studies examining men with persistent post-finasteride syndrome (men who stopped the drug but continued experiencing side effects despite normalized serum hormone levels) found that neurosteroid concentrations in cerebrospinal fluid remained substantially suppressed compared to healthy controls. Allopregnanolone, DHEA, and DHT in the brain’s fluid environment had not recovered even though serum measurements would have told you these men were completely fine.
The implication is profound: a drug can permanently alter the hormonal environment of specific tissues in ways that are completely invisible to systemic blood testing. The brain’s neurosteroid milieu can be disrupted while every blood panel comes back normal.
In scalp follicles, DHT concentrations in actively balding regions are substantially elevated compared to both serum DHT and non-balding regions in the same scalp. Two men with identical serum DHT can have dramatically different androgenic activity in their follicles based on local 5AR expression and androgen receptor sensitivity. This is why some men with high serum DHT never lose hair while others with normal serum DHT go bald, the scalp is operating on its own local biochemistry that serum cannot characterize.
Short of a tissue biopsy (prostate biopsy, scalp punch biopsy, lumbar puncture for CSF), you cannot directly measure what is happening in these compartments. Every systemic test is, at best, an educated inference about tissue-level reality.
The Urinary Hormone Test: The Best Systemic Picture Available
Given all of that, where does urinary hormone metabolite testing sit?
It does not solve the tissue accumulation problem. Nothing short of a biopsy does. But it measures something fundamentally different from blood or saliva. And for specific questions, particularly around enzyme activity and metabolite routing, it is substantially more informative than any serum panel.
What urine measures is what the liver and kidneys have actually processed and cleared over the collection period. Not a snapshot of what is in transit. Not what one gland secreted at one moment. The cumulative enzymatic output of the steroid hormone system across an entire day, captured in the metabolites that result from specific enzymatic steps.
This matters enormously for 5-alpha reductase assessment because of one specific ratio that blood testing cannot provide.
Androsterone versus etiocholanolone. These are the two major terminal metabolites of testosterone and androstenedione after 5-alpha and 5-beta reduction respectively.
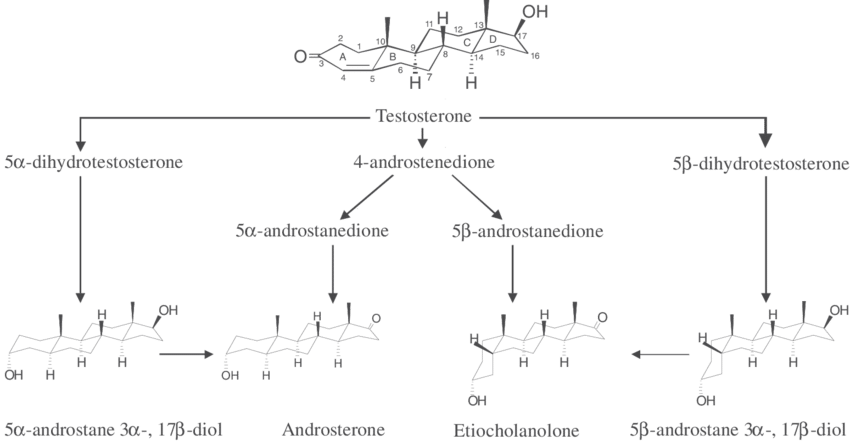
Androsterone is the 5-alpha reduced product → the more androgenic pathway. Etiocholanolone is the 5-beta reduced product → essentially inert as an androgen. The ratio between them is the actual readout of 5-alpha reductase enzymatic preference, independent of how much testosterone substrate was available, independent of what aromatase was doing, independent of DHT clearance rates.
And androsterone is produced at roughly 100 to 200 times the daily urinary volume of DHT.
Let that land for a moment. The metabolite everyone is focused on, DHT, represents less than 1 percent of the total daily androgenic metabolite output measurable in urine. Androsterone, which almost nobody discusses, dwarfs it. If you are trying to assess 5-alpha reductase activity and you are only looking at DHT, you are looking at the smallest part of the picture while ignoring the largest part.
This is the total androgen pool concept. When you add up all measurable urinary androgen metabolites (testosterone, DHT, androsterone, etiocholanolone, androstanediol, 11-hydroxy-androsterone, 11-hydroxy-etiocholanolone, DHEA, DHEAS, androstenedione) you get a number that represents the actual daily androgenic metabolite output of your body. DHT typically represents less than 0.2 percent of that total. Androsterone and etiocholanolone together typically represent 70 to 80 percent.
A true 5-alpha reductase inhibitor does not just lower DHT. It shifts the entire androsterone:etiocholanolone ratio. It changes the total pool composition. If you see DHT go down in a blood test but the AN:ET ratio in urine is unchanged, the enzyme is not actually being inhibited; something else is happening.
The Estrogen Picture No Blood Test Shows You
Now apply the same logic to estrogens. And brace yourself, because this is where the gap between what people measure and what actually matters becomes most stark.
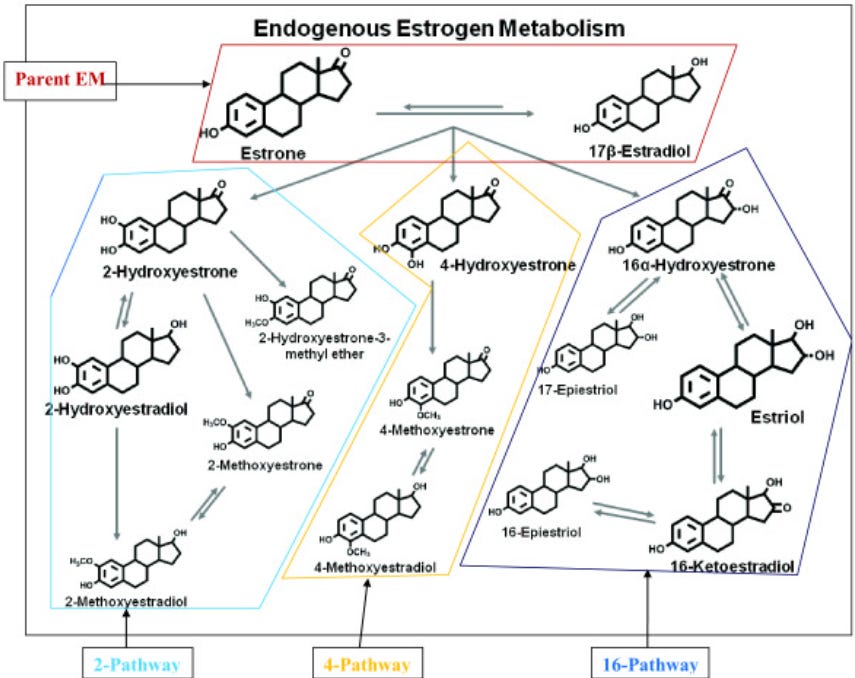
Your body does not simply produce estradiol and call it done. Estradiol and estrone are metabolized through a cascade of enzymatic steps that produces an entirely different family of molecules (catechol estrogens) each with distinct biological activity.
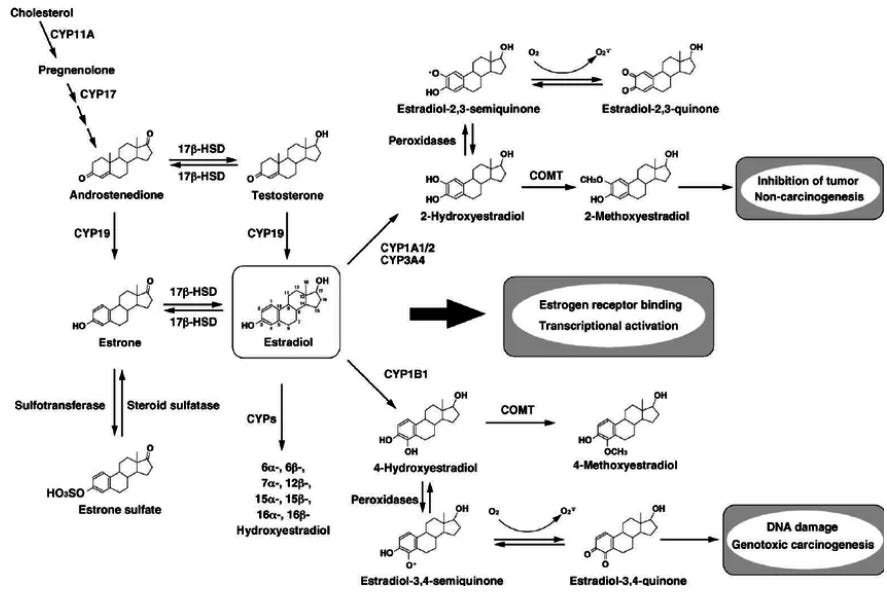
Phase I metabolism routes estrogens down three pathways:
The 2-OH pathway, driven by the enzyme CYP1A1, produces 2-hydroxyestrone and 2-hydroxyestradiol. These are considered the safest estrogen metabolites → anti-proliferative, relatively inert, cleared efficiently. They should represent 40 to 88 percent of your catechol estrogen fraction.
The 4-OH pathway, driven by CYP1B1, produces 4-hydroxyestrone and 4-hydroxyestradiol. These have genotoxic potential → they can form DNA adducts and have been associated with increased cancer risk in breast tissue. They should represent less than 10 percent of the catechol fraction.
The 16-OH pathway, driven by CYP3A4, produces 16-alpha-hydroxyestrone. This metabolite is highly estrogenic → it binds estrogen receptors with high affinity and drives proliferative activity. It should represent 10 to 50 percent of the fraction.
Then there is Phase II → methylation. The enzyme COMT, using magnesium as a cofactor and SAM as the methyl donor, converts the 2-OH and 4-OH catechol estrogens into their methoxy forms, which are inert and ready for safe excretion. The ratio of 2-methoxyestrone to 2-hydroxyestrone tells you how efficiently this is happening. A low ratio means your body is producing the safer 2-OH metabolites but not successfully converting them to their inactive forms, leaving reactive catechol estrogens in circulation longer than ideal.
Two people with identical serum estradiol can have completely different profiles across these ten measurable metabolites. One person routing 80 percent of their catechol estrogens through the 2-OH pathway with efficient methylation. Another person routing 60 percent through the 16-OH pathway with impaired methylation. The same E2 number. Completely different biological reality. Completely different intervention needs. And standard bloodwork cannot distinguish them because it only measures the starting point.
My Wife Has Higher 5-Alpha Reductase Activity Than I Do
This is where the data from my own household becomes the most compelling illustration of everything above.
My wife and I ran simultaneous urinary hormone metabolite panels → the same test, the same laboratory, collected in the same week. I am a 33-year-old male using 500 to 600 milligrams of testosterone enanthate per week. She is a 31-year-old female using no exogenous hormones (except pregnenolone). My testosterone input is roughly 25 to 30 times higher than hers.
Her 5-alpha reductase activity, measured by the androsterone:etiocholanolone ratio across three independent steroid pathways, is higher than mine across every single metric.
Her androgen pathway 5α:5β ratio is above the reference range. Her progesterone pathway 5α:5β ratio is above the reference range. Her cortisol pathway 5α:5β ratio is above the reference range. A systemic 5α preference running through every steroid class her body processes… not driven by her testosterone input, but by intrinsic enzyme expression.
Mine are all within range. Despite feeding the enzyme 25 to 30 times more substrate, my intrinsic 5-alpha reductase activity preference is lower than hers.
And her total androgen pool (adding up every measurable urinary androgen metabolite) is approximately 67 percent of mine, despite receiving a fraction of the exogenous testosterone. Her total estrogen pool is nearly identical to mine in absolute size. But the internal routing of that estrogen pool is completely different. Hers dominated by the highly estrogenic 16-OH pathway, mine dominated by the safer 2-OH pathway. (we’re addressing her ratio now since we tested and know what it looks like)
Identical pools. Completely different compositions. Completely different implications. Completely invisible to standard bloodwork.
This is not a story about pathology. It is a story about individual variation. Enzyme activity is intrinsic. It is written in your genetics, shaped by your metabolic environment, influenced by insulin signaling, thyroid function, body composition, and gut health. Two people on the same compound at proportional doses will have dramatically different hormonal responses based entirely on variables that a testosterone and estradiol blood panel will never surface.
The Confounders Nobody Checks
Before you interpret any hormone test (urinary or otherwise) there are three biological variables that can significantly alter the results and that almost nobody accounts for.
Gut beta-glucuronidase. The liver packages hormone metabolites in a water-soluble form (glucuronidation) to prepare them for excretion in urine and bile. But certain gut bacteria produce an enzyme called beta-glucuronidase that can cleave this packaging in the intestine, allowing hormone metabolites to be reabsorbed into circulation rather than excreted.

Elevated gut beta-glucuronidase means higher effective estrogen recirculation, altered estrogen metabolite profiles, and potentially confounded urinary hormone data. My wife and I both tested beta-glucuronidase on a gut microbiome panel, both on the lower end of the reference range, meaning minimal enterohepatic recirculation and valid urinary hormone data. This is worth checking before interpreting any urinary estrogen metabolite results.
Liver enzyme activity. The liver is where most hormone metabolism happens. Impaired hepatic function alters metabolite production and clearance in ways that would confound urinary hormone results. My liver enzymes at the time of testing were in the 20 to 30 rang, within normal limits, even on injectable testosterone. This confirms that hepatic processing was functioning normally and that the metabolite picture reflects actual enzymatic preferences rather than clearance impairment.
Thyroid function. Thyroid hormone, specifically T3, is a significant upregulator of 5-alpha reductase type 2 expression. Research shows T3 dose-dependently increases 5AR2 gene expression while having minimal effect on 5AR1, meaning that thyroid status directly influences the 5AR side of the equation. A hypothyroid state with low T3 would be expected to reduce 5AR type 2 activity and lower DHT production, while optimal thyroid function supports robust 5AR2 expression. My TSH at the time of testing was 1.6 to 1.9 (optimal range, clearly euthyroid) meaning my thyroid status was not suppressing 5AR activity and is not a confound for the 5AR metabolite picture.
Check these three variables before you interpret your urinary hormone results. They are not optional context… they are validity checks on the data.
What This Means for You
You do not need to run a urinary hormone panel tomorrow. But you do need to update the mental model you use to interpret any hormone data you see. Your own or anyone else’s.
When someone posts their testosterone and DHT on a forum and draws conclusions about their 5-alpha reductase activity, they are looking at one metabolite that represents less than 0.2 percent of the total androgenic output their body is managing, using a ratio that conflates enzyme activity with substrate load and aromatase competition, from a single blood draw that could vary 40 percent depending on when it was taken. The AN:ET ratio, which actually measures 5AR enzymatic preference, is not available from that test and cannot be inferred from it.
When someone posts their estradiol and concludes their estrogen is fine, they are looking at one molecule from a family of sixteen measurable metabolites, with no information about whether that estradiol is being routed through the safest pathway or accumulating as highly estrogenic and potentially genotoxic metabolites, and no information about whether their phase II methylation is converting those metabolites efficiently for excretion.
The hormone optimization community is making protocol decisions based on measurements that capture a small fraction of the relevant biology. This is not an argument against blood testing; it is an argument for understanding what blood testing actually measures and what it does not.
The full picture requires looking at the metabolites, not just the hormones. The ratios, not just the absolute values. The total pool, not just the headline number. And the enzyme activity, not just the substrate.
P.S. I’m not against blood tests at all. I do them myself at least every 2-4 weeks after each experiment. They have a lot of value, but are best used in combination with other tests, like the HuMap (hormone urinary test I did).
What Comes Next
In the next article in this series, I apply everything above to a specific self-experiment.
I ran urinary hormone panels on myself and my wife after using two compounds that are both proposed in natural hormone optimization circles as 5-alpha reductase inhibitors…thymoquinone from black seed oil and Scutellaria baicalensis extract (Chinese skullcap from Nootropics depot). Solid doses of both. High-quality extracts. Simultaneously.
The result was a null. Neither compound, alone or in combination, produced detectable 5-alpha reductase inhibition across any of the metabolite ratios, in me or in my wife.
What the data shows, what it means for the bioavailability question, why my wife’s data is actually the cleaner test case, and what I am doing next → that is Article 2.
Subscribe so you do not miss it. Because if you found this one eye-opening, the next one is where the experiment data gets interesting.
Ask Hans
Still have questions after reading this? Not sure which hormone test is right for you, what your AN:ET ratio means, or where to even start with estrogen metabolism? Ask Hans has been trained on everything I’ve published (protocols, research, clinical frameworks, all of it). It’s like having my entire knowledge base in your corner, available instantly. If you’re stuck, confused, or just want to go deeper on anything covered in this article → Ask Hans.
Personalized Health Report
Reading about hormone metabolism is one thing. Knowing what YOUR hormones are actually doing. And knowing exactly what to do about it is another. Submit your labs, diet, supplements, lifestyle, and health history and I’ll analyze everything personally. No symptom chasing. No generic protocols. A precise roadmap to the root cause, built specifically for you. Get your personalized health report here.
The total androgen pool comparison was wild. What about the pregnenolone having a toll on the comparison? What's the dose?🤔